-
Inner Journeys: Mental Health and Psychosocial Perspectives on the Migration, Return and Reintegration Experiences of Ethiopian, Somali and Sudanese Migrants in Vulnerable Situations
Overview
 This mixed-method study examines the consequences that migration, return and reintegration experiences have on the mental health and the psychosocial well-being of returning migrants, with the primary purpose of informing policies, programmes and advocacy initiatives that promote sustainable reintegration. The study sites included Addis Ababa, Dire Dawa, Jimma, Hossana and Kambata; Khartoum, El-Fasher and Nyala; Mogadishu and Hargeisa .
This mixed-method study examines the consequences that migration, return and reintegration experiences have on the mental health and the psychosocial well-being of returning migrants, with the primary purpose of informing policies, programmes and advocacy initiatives that promote sustainable reintegration. The study sites included Addis Ababa, Dire Dawa, Jimma, Hossana and Kambata; Khartoum, El-Fasher and Nyala; Mogadishu and Hargeisa .
The findings and recommendations are relevant to mental health and psychosocial support (MHPSS) specialists, protection officers and other return and reintegration practitioners.
They can usefully inform the design of interventions specific to the psychosocial dimension of protection and reintegration, as well as the integration of psychosocial considerations into other interventions, including those with a social, economic and health focus.

A number of key findings emerged from the study which generated 11 programmatic recommendations.
Most returning migrant populations reported being in a situation of vulnerability. Despite this, many display great resilience in the face of various challenging experiences.
Recommendation 1 – Reintegration initiatives should take a resilience-based approach, recognizing that with a supportive environment people can and do recover their mental health and well-being. MHPSS activities should identify and encourage the many positive coping strategies and resources that returnees have.

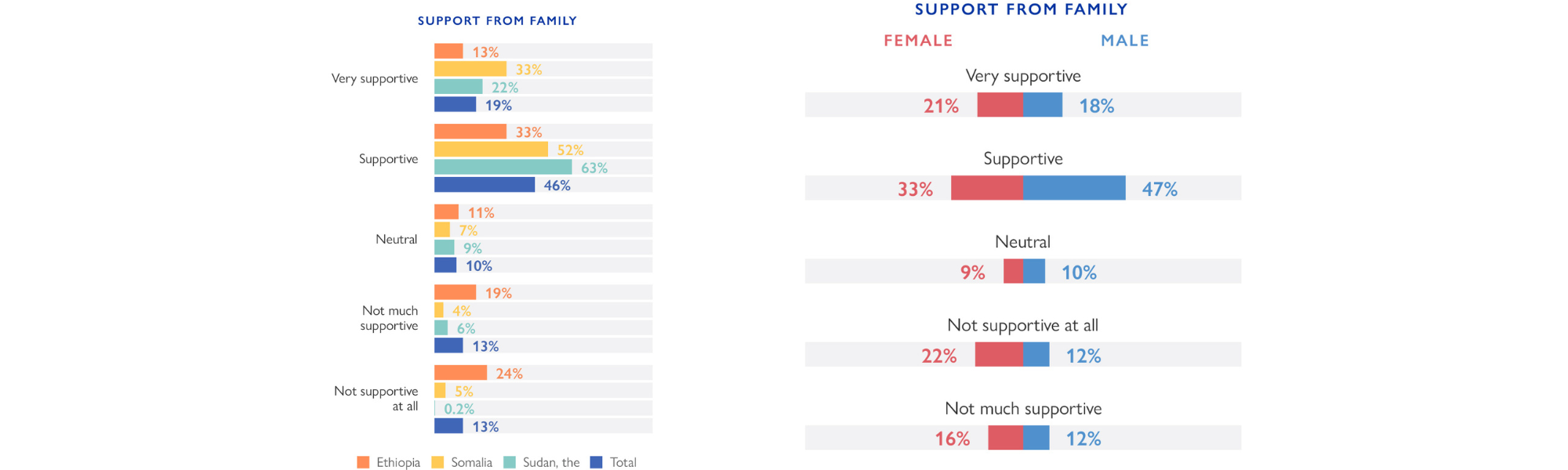
Family support is a key factor that facilitates the reintegration of returning migrants.
Recommendation 2 – Family engagement should be considered as a paramount aspect of reintegration assistance. At minimum, families should be prepared to receive their family member and supported to be welcoming and accepting.
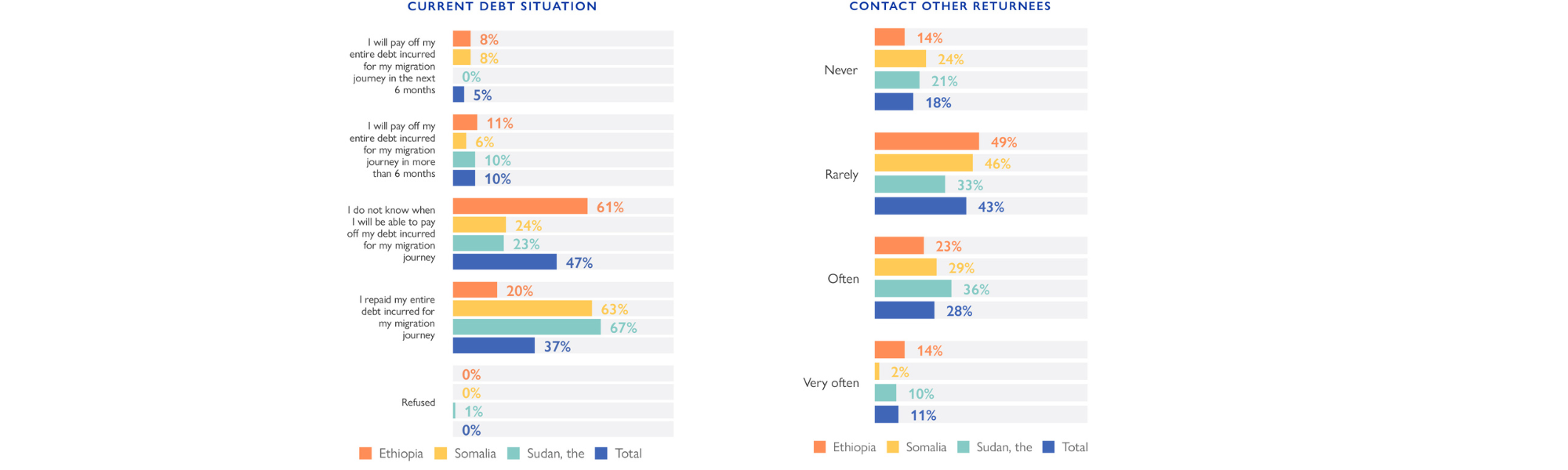
Returnees reported supporting each other in various ways, ranging from teaching each other how to do a certain job, to collecting money among each other to be used when needed.
Recommendation 3 – Returnees should be encouraged to leverage their own social networks as part of their reintegration process, through engaging in community life and other social activities that they enjoy and that connect them with others. This could form part of the reintegration planning process.

Recommendation 4 – Reintegration-related MHPSS activities should include the organization of peer support and strengthen/create community committees when appropriate. These activities need to be properly planned and budgeted for. Other community-based activities, such as sociorelational and cultural activities, creative and art-based activities, rituals and celebrations, sports and play, and informal learning should be organized by MHPSS teams to support social cohesion between community members and to foster a sense of collective identity. It is important to consider that returnee-only activities may have adverse effects on stigmatization.
The psychosocial counselling sessions provided by IOM are useful in helping returnees regain hope and motivation.
Recommendation 5 – The provision of individualized psychosocial counselling sessions, alongside community-level MHPSS activities and other social and economic forms of assistance, should continue as part of return and reintegration support.

Unmet basic needs result in a deterioration of psychosocial well-being.
Recommendation 6 – The reintegration process should focus, especially in the initial stages, on meeting basic needs, including food, housing, clothing and medical care. Reintegration programmes should assess whether returning migrants can meet their basic needs and map actors that can intervene as needed. MHPSS service providers engaged in reintegration activities should advocate for the basic needs of the people they support to be met and ensure a close connection with other reintegration services/service providers.
A lack of ‘psychological readiness’ and unrealistic expectations may be linked for some returnees to the inability of fully benefiting from economic reintegration assistance. The need for a stronger linkage between MHPSS interventions, vocational training, formal and informal education and economic reintegration was evident.
Recommendation 7 – To strengthen the effectiveness and impact of economic reintegration initiatives aiming primarily for returnees to meet their own basic needs in the long run, there is a need to integrate MHPSS approaches and principles.

Access to MHPSS services is severely limited in Ethiopia, Somalia and the Sudan.
Recommendation 8 – There is a need to advocate for more investment in human and financial resources on MHPSS at the national level within Ethiopia, Somalia and the Sudan. In the health sector, funds should diversify away from only supporting psychiatric institutions towards also supporting community-based care, addressing social determinants of mental health and developing more community-based interventions. Training should be offered to existing MHPSS services on human mobility dimensions and how they can best serve migrants.
Many returnees had no or little contact and/or knowledge of any kind of MHPSS service providers.
Recommendation 9 – The impact of challenging migration and return experiences on the mental health and psychosocial well-being of returning migrants requires actors to develop culturally sensitive interventions. Given the stigma around people with mental health problems and its hindering effects on help-seeking behaviour, sensitization sessions on psychosocial well-being are vital to address this issue. In order to mobilize community resources, community leaders including religious leaders should be involved in such activities and given active roles in conveying messaging to community members.
The standards of mental health care are generally low, especially for patients with psychotic symptoms.
Recommendation 10 – A thorough assessment of the quality benchmarks of MHPSS services should be done before referrals are made. These can be based on the World Health Organization Quality Rights toolkit and should cover issues such as staff capacity and types of psychiatric drugs available, and for inpatient facilities, the availability of food, water and adequate accommodation facilities. As far as possible, return and reintegration stakeholders should support referral partners to address these gaps to bring their care up to standard, for example through staff training or the provision of drugs, supplies and equipment.

Services provided should address the specific vulnerabilities and needs of different groups, such as women and child returning migrants, or children of adult returning migrants. The experiences of the latter two groups remain largely understudied.
Recommendation 11 – Future research should identify the short- and medium-term reintegration experiences and needs of returned children. Reintegrating programming should provide child-friendly services and, where possible, include these into referral systems. Further research on the children of adult returning migrants should also be encouraged.